Inflammatory Bowel Disease (IBD) has always been a moving target for doctors and patients alike. For years, the goal was simply to stop the bleeding and reduce pain. But today, we have moved beyond managing symptoms. We are talking about healing the gut lining and stopping the damage before it starts. This shift happened because of targeted therapies known as IBD Biologicsa class of medications that use proteins to interrupt specific parts of the immune system responsible for inflammation in the gut.. If you are navigating a diagnosis of Crohn’s disease or Ulcerative Colitis, you’ve likely heard terms like Anti-TNF or IL-23 throw around during appointments. These sound like acronyms from another planet, yet they represent your daily lifeline to normalcy.
The landscape of treatment has shifted dramatically since the late 1990s. Back then, options were limited to steroids that made you feel bloated and jittery. Now, we have precision tools. As of early 2026, approximately 3 million Americans rely on these medications. The big question remains: which one fits your life? Do you want the fastest relief or the safest long-term profile? Let's break down exactly how these three main families work, who they help most, and what it truly feels like to live on them.
Understanding the Core Mechanism
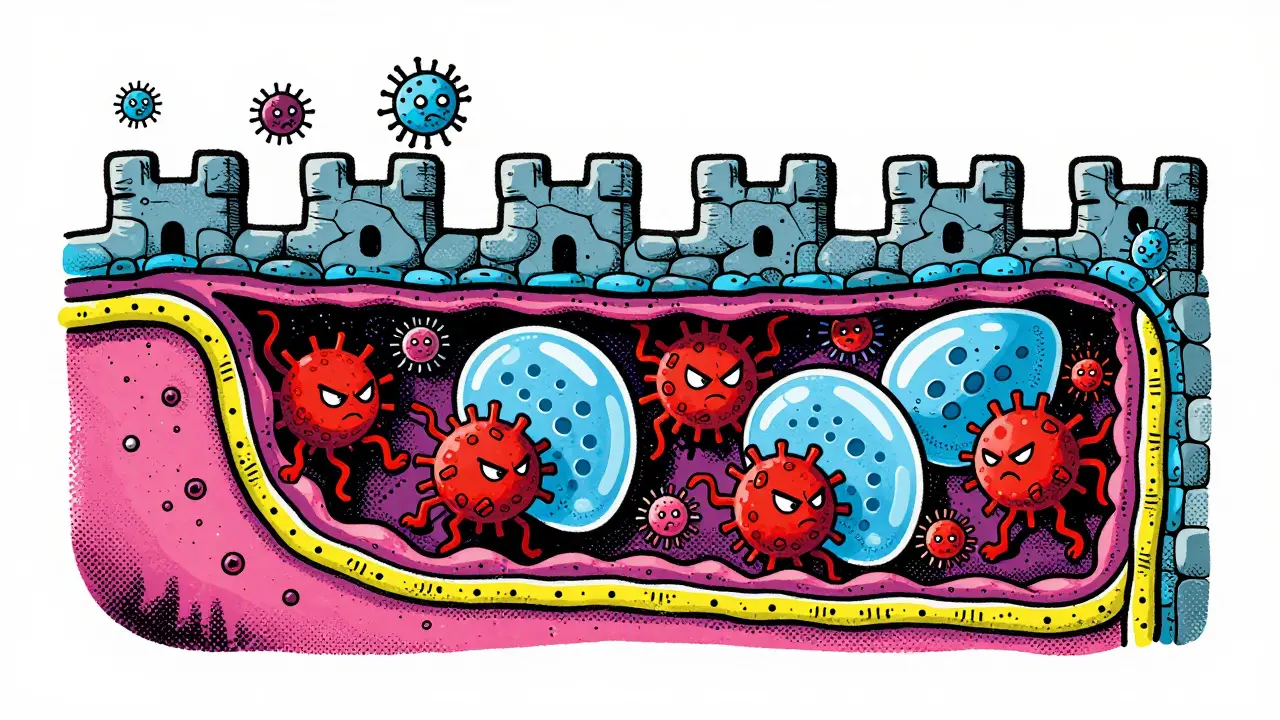
Before picking a drug, you need to know what it attacks. Your immune system is designed to fight infections, but in IBD, it mistakenly attacks your own intestine. Think of your gut lining as a castle wall. In a healthy person, bacteria outside the castle stay out. In IBD, the wall gets porous, and the immune system sends in troops-specifically proteins called cytokines-to attack what it thinks is an enemy.
Biologics work by blocking these specific signals. Unlike standard immunosuppressants that lower your entire defense system (making you susceptible to every cold and flu), biologics are surgical strikes. They zero in on one pathway. For instance, some block Tumor Necrosis Factor (TNF), a fiery signal that causes swelling. Others stop cells from migrating into the gut tissue, while newer ones cut off the supply of interleukins, the chemical messengers that keep the fire burning.
According to the Crohn's & Colitis Foundation, these agents mimic natural body proteins to 'turn down' the mistaken immune response targeting the gastrointestinal tract.The Original Heavy Hitters: Anti-TNF Agents
You cannot discuss IBD treatment without starting with Anti-TNF agents. These were the first generation of biologics and remain the gold standard for inducing rapid remission in severe cases. The two main players here are Infliximab (Remicade) and Adalimumab (Humira).
Infliximab is an intravenous medication. You get it in a clinic over a few hours. It works fast, often showing improvement within days. Data from network meta-analyses consistently ranks Infliximab highly for mucosal healing-meaning it closes the ulcers in your bowel lining-which is crucial for preventing future complications. However, because it targets a protein found throughout your body, not just the gut, it carries a higher risk of systemic side effects. Studies suggest a 30-50% higher rate of serious infections compared to standard care. That said, biosimilars like Inflectra and Cyltezo have made this option significantly cheaper than it was a decade ago.
Adalimumab changed the game by introducing convenience. You inject it under your skin yourself. This means fewer trips to the hospital and more control over your schedule. While studies show it might be slightly less potent for immediate induction than Infliximab, many patients find the quality-of-life benefits worth the trade-off. About 87% of patients successfully manage self-injections after training. It’s particularly popular for maintaining remission once the flare is under control.
| Comparison of Top Anti-TNF Medications | ||
|---|---|---|
| Feature | Infliximab (Remicade) | Adalimumab (Humira) |
| Delivery Method | Intravenous (IV Infusion) | Subcutaneous Injection |
| Induction Dose Schedule | Weeks 0, 2, and 6 | High dose initially, then every other week |
| Typical Cost (Single Dose) | $3,000 - $8,000 | $3,000 - $5,000 |
| Speed of Relief | Rapid (2-4 weeks) | Moderate (4-8 weeks) |
The Gut-Specific Warriors: Anti-Integrin Therapy
If you worried about the systemic risks of Anti-TNF agents, there is a smarter alternative. Enter Vedolizumab (Entyvio). This drug works differently. Instead of blocking a chemical messenger, it blocks the "doors" white blood cells use to enter your intestines. It binds to alpha-4 beta-7 integrin receptors.
Why does this matter? Because this mechanism is highly specific to the gut. Other tissues in your body aren’t affected nearly as much. For patients with a history of multiple sclerosis (MS) or latent tuberculosis, this selectivity is vital. Data indicates a significantly cleaner safety profile compared to TNF blockers. One study showed the risk of PML (a rare brain infection associated with natalizumab) was extremely low for Vedolizumab. The trade-off is speed. Vedolizumab can take 6-10 weeks to reach full effect. It’s not the drug you reach for when you’re in agony today; it’s the drug you choose when you want stability tomorrow without constant worry.
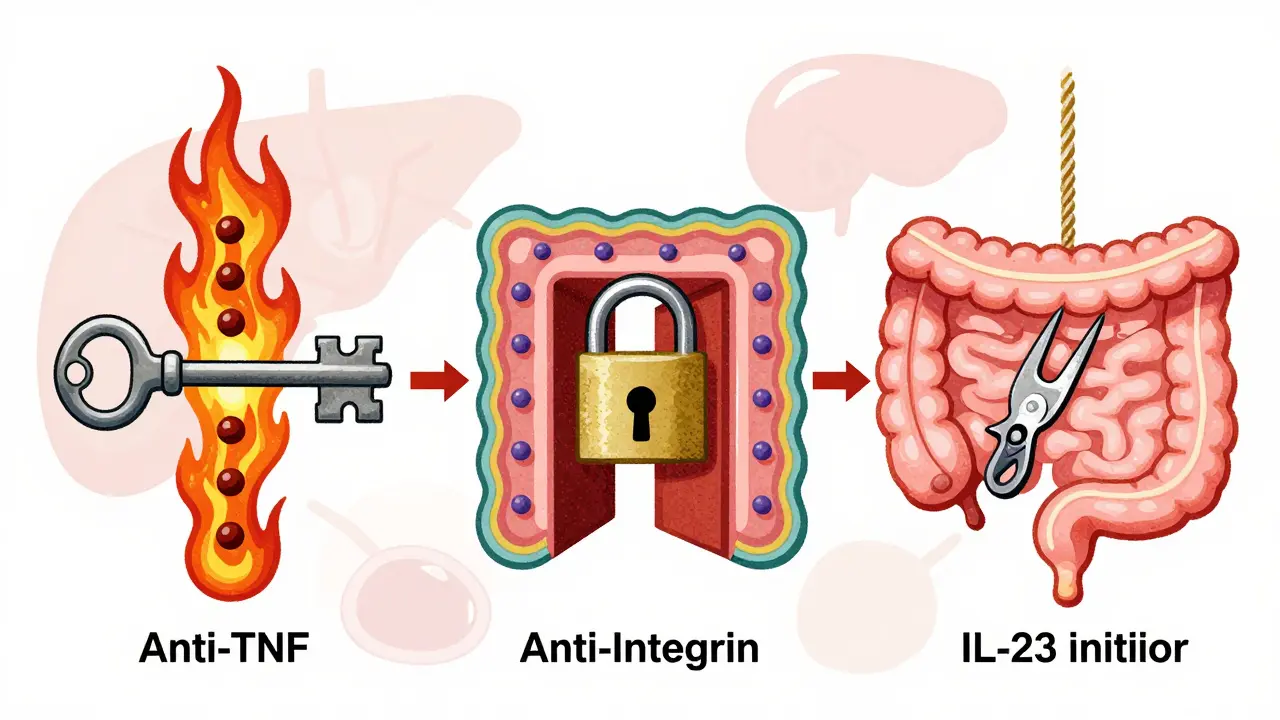
The New Guard: Interleukin Inhibitors
By 2026, the most exciting developments belong to Interleukin (IL) inhibitors. These drugs target pathways even later in the inflammatory chain. Specifically, they block IL-12, IL-23, and sometimes IL-6.
Ustekinumab (Stelara) targets both IL-12 and IL-23. Originally used for psoriasis, it revolutionized Crohn’s care. It offers a long dosing interval (every 8 to 12 weeks), which reduces needle fatigue. Recent approvals have expanded its use to Ulcerative Colitis as well, solidifying its place as a versatile maintenance agent.
Then comes the blockbuster of the year: Risankizumab (Skyrizi). Approved for Ulcerative Colitis in mid-2024 following the ADVENT trial results, it became the first IL-23 inhibitor to claim success in both Crohn’s and UC. Trials showed clinical remission rates near 30%, beating placebo decisively. Another newcomer is Mirikizumab (Omvoh), which targets a specific part of the p19 subunit of IL-23. Early feedback from patient communities highlights fewer infusion reactions and injection site issues compared to older biologic generations.
Comparing Efficacy and Patient Experience
Picking a biologic isn't just about looking at charts; it's about reading real lives. A 2024 survey across patient forums revealed distinct patterns. Those on Anti-TNF reported feeling better faster-sometimes within a week-but complained about the rigidity of clinic schedules and the fear of "antibody formation." Over time, your body can recognize a biologic as foreign and build antibodies against it, rendering the drug useless. This happens in roughly 25% of Anti-TNF users. Combining it with oral meds like Azathioprine can reduce this risk, adding complexity.
Conversely, patients on Vedolizumab report high satisfaction regarding peace of mind, even if the start is slower. One user on MyIBDTeam described switching to Vedolizumab after five years on Humira: "No more weekly injections but had to wait 10 weeks for full effect, which was brutal." On the flip side, the IL-23 group often cites the dosing frequency as their biggest win. Getting a shot once a month rather than twice a week changes your relationship with your treatment entirely.
Financial reality checks are equally important. While biosimilars have lowered prices for older drugs, costs remain steep. As of Q2 2024 data, a single infusion of Vedolizumab ran around $5,500. Most insurance plans have tier structures. Manufacturer assistance programs like Janssen CarePath often bridge the gap for eligible patients, frequently bringing out-of-pocket costs down to nominal amounts. Never start a regimen without verifying your coverage status first, as denials can leave you scrambling in the middle of a flare.

Choosing the Right Path Forward
There is no single "best" drug. The AGA Technical Review suggests that for bio-naive patients (those never treated with biologics) suffering moderate-to-severe disease, Infliximab often holds the edge in strength. Dr. Adam Cheifetz noted in 2023 that the evidence base for Infliximab is simply deeper. However, if you have co-existing conditions like psoriasis or rheumatoid arthritis, an Anti-TNF might be contraindicated or less suitable due to potential exacerbation of certain autoimmune symptoms.
If your priority is avoiding systemic infections, Vedolizumab becomes the preferred starting point. For those already fatigued by frequent shots, Ustekinumab or Risankizumab offers a streamlined schedule. Always remember, monitoring is key. Regular blood work tracks liver function and drug levels. If you are on an Anti-TNF, watching for antibody levels is standard practice to preempt loss of response.
Frequently Asked Questions
Can I switch biologics if one stops working?
Yes, absolutely. Many patients rotate through different classes. If an Anti-TNF fails, switching to an integrin inhibitor or IL-23 inhibitor is common. Success rates tend to drop slightly with sequential use, but effective remission is still very achievable in subsequent lines of therapy.
Are biologics considered curative for Crohn's or UC?
They induce remission, not a permanent cure. The goal is deep remission (no inflammation visible on colonoscopy) for long periods. However, they prevent complications like strictures or surgery. If you stop the medication, symptoms almost invariably return eventually.
Do I need vaccines before starting these drugs?
Yes, you should be up to date on all non-live vaccines. Live vaccines (like MMR or Varicella) are dangerous when combined with these powerful immunosuppressants. Discuss your vaccine history with your gastroenterologist immediately before starting treatment to boost immunity beforehand.
Is there a difference between generic biologics and biosimilars?
Biosimilars are highly similar versions of the original drug, not simple chemical copies like generic pills. They go through rigorous testing to prove safety and efficacy equivalent to the brand name. They are generally interchangeable and significantly more affordable.
How long does it take to see results?
Timing varies by drug class. Anti-TNF agents (Infliximab) often work within 2-4 weeks. Anti-integrins (Vedolizumab) typically take 6-10 weeks for full effect. Newer IL-23 inhibitors (Risankizumab) usually show significant benefit within the first 4-12 weeks depending on the severity of inflammation.

sanatan kaushik
March 30, 2026 AT 00:35The prices listed for Infliximab are insane for people in India but maybe okay for Americans. We rely on older meds because nothing new works without insurance coverage. The gap between what the paper says and what reality feels like is huge. You cannot ignore the economic barrier here.
Ruth Wambui
March 31, 2026 AT 19:14They sell us poison wrapped in protein chains while the real cure is buried in soil amendments nobody studies anymore. The FDA just wants to clear their inbox before the next election cycle rolls around. Corporate interests drive the approval timeline far more than actual patient recovery metrics ever could.
Carolyn Kask
April 1, 2026 AT 22:57Stop romanticizing the failure of clinical trials and admit the government approves garbage just to keep stock prices up. It is a scam designed to drain the healthcare budget dry. Your optimism is actually dangerous in this environment.
Christopher Curcio
April 1, 2026 AT 23:52We need to discuss the pharmacokinetics of p19 subunit binding versus full p19 blockade regarding mucosal healing rates. The data suggests that selective inhibition reduces off-target effects significantly compared to broad TNF suppression. Monitoring antibody titers remains crucial for preventing secondary non-response during maintenance phases of treatment.
Katie Riston
April 3, 2026 AT 12:21Everyone waits for the medicine to kick in but nobody talks about the limbo phase. The waiting sucks because you never know if you are recovering or dying slowly. You plan your week around infusions and hospital visits become the only constant routine. It feels like prison time where the guards hold the keys to your health. Some drugs work fast while others drag the process out for weeks or months. Months feel like years when you are sick and living with unpredictable flare-ups. Pain changes how you see the future so you stop making plans beyond the next injection. Hope is the only currency left when your body betrays you every morning. Insurance adds another layer of anxiety on top of the physical suffering you endure daily. Denials happen in the worst moments when you thought you had finally found a rhythm. Appearances matter less than stability since hiding symptoms drains energy you need elsewhere. Silence becomes a survival skill in social situations where admitting weakness invites judgment from outsiders. We survive until the next shot keeps the fire down inside the gut lining. Nobody prepares you for the mental toll of relying on proteins to hold your body together.
emma ruth rodriguez
April 5, 2026 AT 00:11Indeed, the pharmacological distinction between biosimilars and originators is critical for patient safety profiles, therefore we must remain vigilant regarding immunogenicity risks throughout treatment duration. The evidence supports careful monitoring of drug levels to ensure therapeutic efficacy.
Beccy Smart
April 5, 2026 AT 16:33I hate needles 😭 why not pills 💊💉😩 tired of injections 🤦♀️ hope they find magic candy 🍬🍬🥺
Jonathan Sanders
April 7, 2026 AT 15:09Oh wow, imagine waking up feeling alive instead of constantly bleeding into your pants for fun. Your complaints sound adorable coming from someone who hasn't faced true adversity yet. I am tired of hearing about needle fatigue when some of us bleed internally every night.
Angel Ahumada
April 8, 2026 AT 01:10the mechanism described ignores the holistic energy field surrounding our digestive tracts yet it seems effective for the masses who lack awareness. Science misses the spiritual component of healing entirely. People who focus on chemistry miss the soul connection.
Rick Jackson
April 8, 2026 AT 15:42Peace comes from managing expectations regardless of the molecule used. Acceptance allows for better quality of life even with chronic conditions present.
Biraju Shah
April 9, 2026 AT 06:11Insurance tiers decide health outcomes more than biology does in this country. The algorithmic denial processes prioritize profit over human suffering consistently. We need systemic reform instead of just better drugs that nobody can afford.
Cameron Redic
April 9, 2026 AT 08:35Your naivete is cute but the financial burden destroys families faster than colitis does. Savings accounts get emptied within months of diagnosis for most working class patients. Charity care ends quickly when the paperwork gets lost in bureaucratic hell.
Calvin H
April 9, 2026 AT 14:48Money talks and everything else walks away from the table.
Debbie Fradin
April 10, 2026 AT 03:11Look on the bright side, at least cancer isn't the only thing costing thousands now. The silver lining is that at least the insurance sometimes covers half. I guess you are winning the lottery of bad diseases if you get UC instead of something silent.
Calvin H
April 11, 2026 AT 10:26It doesn't help when you lose your job because the doctor's notes look bad to HR.